 Gas is another topic most people don’t think much about until they have a newborn. Then suddenly gas becomes a huge source of parental distress, even though parents are not the ones with the gas. It’s the poor newborn baby who suffers, and as all parents know, our children’s suffering becomes OUR suffering.
Gas is another topic most people don’t think much about until they have a newborn. Then suddenly gas becomes a huge source of parental distress, even though parents are not the ones with the gas. It’s the poor newborn baby who suffers, and as all parents know, our children’s suffering becomes OUR suffering.
So what to do?
First, I reassure you that ALL young babies are gassy. Yes, all. But some newborns are not merely fussy because of their gas. Some become fussy, ball up, grunt, turn red, wake up from a sound sleep, and scream because of their gas. In other words, some babies really CARE about their gas.
Remember, newborns spend nine months as a fetus developing in fluid, and have no experience with air until they take their first breath. Then they cry and swallow some air. Then they feed and swallow some air. Then they cry and swallow some more air. Eventually, some of the air comes up as a burp. To summarize: Living in Air=Gas Production.
Gas expelled from below comes from a different source. As babies drink formula or breast milk, some liquid in the intestines remains undigested, and the normal gut bacteria “eat” the food. The bacteria produce gas as a byproduct of their eating. Thus: a fart is produced.
The gas wants to escape, but young babies are not very good at getting out the gas. Newborns produce thunderous burps and expulsions out the other end. I still remember my bleary-eyed husband and I sitting on the couch with our firstborn. On hearing a loud eruption, we looked at each other and asked simultaneously, “Was that YOU?” Then looked at our son and asked “Was that HIM?”
Gas is a part of life. If your infant is feeding well, gaining weight adequately, passing soft mushy stools that are green, yellow, or brown but NOT bloody, white, or black (for more about poop, see our post
The Scoop on Poop), then the grunting, straining, turning red, and crying with gas is harmless and does not imply that your baby has a belly problem or a formula intolerance. However, it’s hard to see your infant uncomfortable.
Here’s what to do if your young baby is bothered by gas:
- Start feedings before your infant cries a long time from hunger. When infants cry from hunger, they swallow air. When a frantically hungry baby starts to feed, they will gulp quickly and swallow more air than usual. If your infant is wide awake crying and it’s been at least one or two hours from the last feeding, try to quickly start another feeding.
- Burp frequently. If you are breastfeeding, watch the clock, breastfeed for five minutes, change to the other breast. As you change positions, hold her upright in attempt to elicit a burp, then feed for five more minutes on the second breast. Then hold your baby upright and try for a slightly longer burping session, and go return her to the first breast for at least five minutes, then back to the second breast if she still appears hungry. Now if she falls asleep nursing, she has had more milk from both breasts and some opportunities to burp before falling asleep.
- If you are bottle feeding, experiment with different nipples and bottle shapes (different ones work better for different babies) to see which one allows your infant to feed without gulping too quickly and without sputtering. Try to feed your baby as upright as possible.
- Hold your infant upright for a few minutes after feedings to allow for extra burps. If a burp seems stuck, lay her back down on her back for a minute and then bring her upright and try again.
- To help expel gas from below, lay her on her back and pedal her legs with your hands. Give her tummy time when awake. Unlike you, a baby can not change position easily and may need a little help moving the gas out of their system.
- If your infant is AWAKE after a feeding, place her prone (on her belly) after a feeding. Babies can burp AND pass gas easier in this position. PUT HER ONTO HER BACK if she starts to fall asleep or if you are walking away from her because she might fall asleep before you return to her. Remember, all infants should SLEEP ON THEIR BACKS unless your infant has a specific medical condition that causes your pediatrician to advise a different sleep position.
- Parents often ask if changing the breast feeding mother’s diet or trying formula changes will help decrease the baby’s discomfort from gas. There is not absolute correlation between a certain food in the maternal diet and the production of gas in a baby. However, a nursing mom may find a particular food “gas inducing.” Remember that a nursing mom needs nutrients from a variety of foods to make healthy breast milk so be careful how much you restrict. Try any formula change for a week at a time and if there is no effect on gas, just go back to the original formula.
- Do gas drops help? For flatulence, if you find that the standard, FDA approved simethecone drops (e.g. Mylicon Drops) help, then you can use them as the label specifies. If they do not help, then stop using them.
The good news? The discomfort from gas will pass. Gas discomfort typically peaks at six weeks and improves immensely by three months. At that point, even the fussiest babies tend to mellow. The next time your child’s gas will cause you distress won’t be until he becomes a preschooler and tells “fart jokes” at the dinner table in front of Grandma. Now THAT is a gas.
Julie Kardos, MD with Naline Lai, MD
©2011 Two Peds in a Pod®

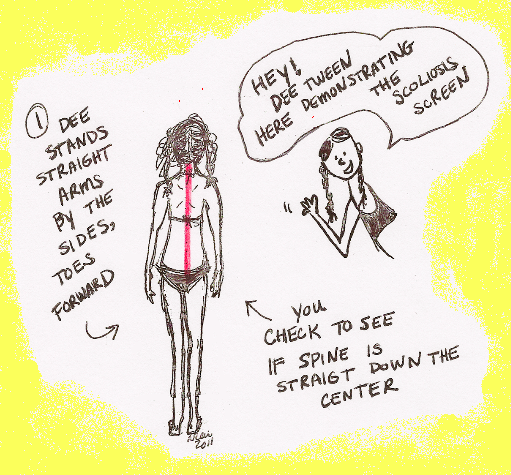



 I remember during my middle school days in New Jersey lining up once a year at the school nurse’s office, feeling awkward and nervous. Not only was the nurse checking our height and weight as she did every year in grade school, but now she was going to check our backs for some mysterious entity called “scoliosis.” Where I live now in Pennsylvania, many school nurses also screen students for scoliosis, a curve in the spine.
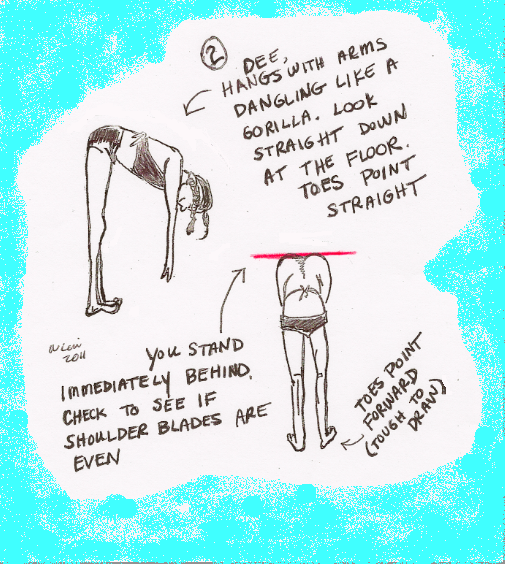
I remember during my middle school days in New Jersey lining up once a year at the school nurse’s office, feeling awkward and nervous. Not only was the nurse checking our height and weight as she did every year in grade school, but now she was going to check our backs for some mysterious entity called “scoliosis.” Where I live now in Pennsylvania, many school nurses also screen students for scoliosis, a curve in the spine.  Depending on the degree of the curve, a child with idiopathic scoliosis might be re-examined every 4-6 months, might get an x-ray of her spine, or her health care provider might refer her to an orthopedic doctor, a specialist who cares for kids with scoliosis. Kids whose spinal curves are severe or are likely to get worse may need bracing until they stop growing. At that point the chances of the curve continuing to increase is low. Wearing a brace does not correct the curve; rather, it prevents any further curvature. Scoliosis braces are much more inconspicuous now than in the past, and can be hidden easily under clothing. Some children require surgery to correct a severe curve.
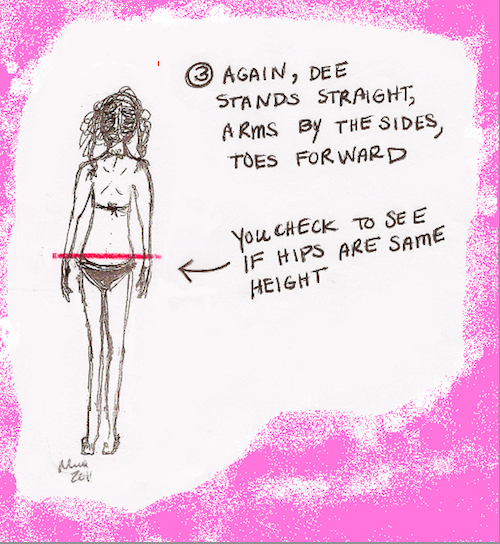
Depending on the degree of the curve, a child with idiopathic scoliosis might be re-examined every 4-6 months, might get an x-ray of her spine, or her health care provider might refer her to an orthopedic doctor, a specialist who cares for kids with scoliosis. Kids whose spinal curves are severe or are likely to get worse may need bracing until they stop growing. At that point the chances of the curve continuing to increase is low. Wearing a brace does not correct the curve; rather, it prevents any further curvature. Scoliosis braces are much more inconspicuous now than in the past, and can be hidden easily under clothing. Some children require surgery to correct a severe curve. 
 I just watched “The Miracle Worker” with my oldest son. This classic 1962 movie depicts Helen Keller, who was deaf and blind, struggling to understand language, with the help and supreme patience of her determined teacher Annie Sullivan.
I just watched “The Miracle Worker” with my oldest son. This classic 1962 movie depicts Helen Keller, who was deaf and blind, struggling to understand language, with the help and supreme patience of her determined teacher Annie Sullivan. 
 If you were around the New York area ten years ago on September 11, you know it was a beautiful crystal-clear day. It was the kind of day which made you gaze admiringly at the sky as you stepped out the door. No one knew that soon the sky over New York, Pennsylvania, and Washington, DC would be marred by the dark clouds of terrorist attacks. Many of your children were too young to remember much about the day, or perhaps they were not even born yet.
If you were around the New York area ten years ago on September 11, you know it was a beautiful crystal-clear day. It was the kind of day which made you gaze admiringly at the sky as you stepped out the door. No one knew that soon the sky over New York, Pennsylvania, and Washington, DC would be marred by the dark clouds of terrorist attacks. Many of your children were too young to remember much about the day, or perhaps they were not even born yet.  Special thanks to Lu Lu of
Special thanks to Lu Lu of  Wondering what crawled into your child’s room and bit her in the middle of the night? If you see two little pinpricks side by side, it’s probably a spider. Spider fangs make two little bite marks. Unfortunately, by the time you examine it in the morning, the bite may be so puffy and red that the two marks are no longer visible. With the exception of the Black widow spider and the Brown recluse spider, most spider bites are harmless and cause only a little bit of irritation. Over-the-counter hydrocortisone 1% ointment, ice, and an analgesic such as acetaminophen or ibuprofen can take the edge off of the itch and/or pain.
Wondering what crawled into your child’s room and bit her in the middle of the night? If you see two little pinpricks side by side, it’s probably a spider. Spider fangs make two little bite marks. Unfortunately, by the time you examine it in the morning, the bite may be so puffy and red that the two marks are no longer visible. With the exception of the Black widow spider and the Brown recluse spider, most spider bites are harmless and cause only a little bit of irritation. Over-the-counter hydrocortisone 1% ointment, ice, and an analgesic such as acetaminophen or ibuprofen can take the edge off of the itch and/or pain.